ANP End Of Year Report
Happy New Year! We hope you enjoyed the holiday season. The New Year will see us hit the ground running, and build on the success of our activities in 2023 to support our
multiple disciplines, including Herbal Medicine, Nutritional Therapy, Health Coach, Acupuncture and Homeopathy.
Read More
In conjunction with the government agency Skills for Heath, the GNC has developed National Occupational Standards for Naturopathic Practitioners. These standards cover practical skills and ethical standards. Practitioners registered with the GNC work within these standards.
Today the ANP is fully engaged with governmental discussions that are of extreme significance to the future of naturopathic practitioners, affecting the access and use of supplements, herbal medicines, homeopathic remedies as well as the health and rights of the wider public. Our message is simple: ANP practitioners help people, and people will benefit from ANP practitioners. The ANP aims to create unity within the profession, to support practitioners and to invest in delivering positive health messages to the public as one unified voice. The Association believes that to support practitioners is to support the growth of the profession, the consequence of which is the embedding of Natural Health into the wider health culture of the UK and Ireland.
Key areas of focus for 2024:
Building a strategy to protect our profession.
In 2024, ANP political will be focusing on lobbying policymakers on laws in the making that will influence Natural Therapies. We are already in communication with key bodies about recognising the value of additional types of evidence beyond the unhelpful RCT model. This follows NICE’s ongoing investigation into how other categories of evidence, such as real-world data, should be used in practice. We will keep you posted on how this conversation develops.
Forging connections with like-minded groups.
To consolidate our position in healthcare, we will continue to advocate for our members with well-connected groups, including the Integrated Health Collaborative and Integrated Medicine Alliance. Working together gives us more power to lobby MPs and the government to change how healthcare is delivered in the UK.
Practically, we are ensuring ANP practitioners are known to social prescribers in GP practices. These are the professionals who can signpost to care outside the NHS. GPs are not allowed to refer to privately named practitioners, but the social prescriber can spotlight helpful therapies and associations representing them. We are working to influence funding decisions made by Integrated Care Boards (previously Clinical Commissioning Groups) to allow patients to access Natural Therapies without having to self-fund. We are learning from the achievements of other groups (e.g., hypnosis for IBS, reflexology for cancer pain) to achieve this.
Furthermore, we have started forming an in-house legal team to consult on matters that could impact our industry so we can be at the forefront of changes to ensure the best outcome to protect the future of our members.
Education and cutting-edge CPD.
In 2024, we will be extending our CPD programme to regional areas of the UK and Ireland to foster community and support for our practitioner members. We will continue to provide our online CPD services, including webinars and mentoring that support clinical development and learning for our members. We have already started engaging keynote speakers for our 6th Annual Summit, scheduled for the 14th and 15th of September, under the theme of chronic pathologies and complex conditions. Next year will also see our first Dublin Summit to support our Irish members.
Dedicated Herbal Medicine support.
In 2024, we will be launching a new initiative to support the various sub-modalities within ANP. This includes herbalists, who like our other members provide an invaluable contribution to medicine. In 2024, herbal medicine practitioners will start seeing more dedicated CPD, business mentoring, support networks and community building to ensure herbalists thrive as practitioners and grow awareness of herbal medicine amongst the public.
Strengthening our community within ANP.
In the New Year, we will be adding more benefits to our association to support our members professionally. In early 2024, we will be launching The ANP Business Club which is being developed to support the business needs of running a clinic and thriving in practice. We will also be encouraging members to use and discuss cases on our closed ANP Facebook group as a means to build practitioner discussions and support more inexperienced practitioners. Lastly, in 2023, we started a new project to rebuild our popular Contraindications Database which will be completed in early 2024. After the completion of the database rebuild, we intend on adding additional drugs and nutraceuticals as an ongoing project and professional resource for both students and full members. Our commitment to having our own database stems from our values surrounding the pharmaceutical industry, and the fact that popular databases, such as The Natural Medicines Database, are owned and produced by Big Pharma.
Proteolytic Degradation of Spike Protein using Natural Therapies
Chronic disabling symptoms from “long COVID” and following mRNA injections are an increasingly prevalent problem. The symptomatic presentation has many common features, which might be explained by the spike protein of the virus, which is also manufactured by the vaccine’s own cells. There is no accepted protocol for treatment. Based on their mechanisms of action, a combination of nattokinase, bromelain, and curcumin should be considered.
Meet the GNC
The General Naturopathic Council (GNC) is the UK regulator for Naturopathy consisting of eleven associations, including the ANP and lay committee members (consumers) working towards an agreed set of aims and objectives.
Read More
In conjunction with the government agency Skills for Heath, the GNC has developed National Occupational Standards for Naturopathic Practitioners. These standards cover practical skills and ethical standards. Practitioners registered with the GNC work within these standards.
The GNC does not offer individual practitioner memberships, and practitioners can only be members via The Association of Naturopathic Practitioners (ANP). GNC registered practitioners have completed a high standard of training that typically involves a 3-year program averaging 3600 hours of educational training and clinical experience. In addition, naturopathic practitioners registered with the GNC agree to abide by a strict code of conduct and ethics.
The GNC has a long-standing reputation as a resource for members of the public seeking highly qualified practitioners under the ‘Find a Practitioner’ page.
ANP Meets with HRH The Prince of Wales
On Wednesday 4th May 2022, the ANP were one of the representatives of the IMA that met with HRH The Prince of Wales at Clarence House in London to discuss the future of natural medicine.
Read More
ANP is one of the founding members supporting the Integrated Medicine Alliance (IMA), initiated by the College of Medicine chair, Dr Michael Dixon, alongside colleagues Dr Naveed Akhtar and Dr Toh Wong. The IMA sets out to inform, educate, and enable access to qualified clinicians in natural therapies, as quoted by Dr Michael Dixon:
“Integrated medicine is so much about what people can do for themselves and each other and their communities both in healing and in enabling people and communities to be more resilient. It allows GPs to apply art and science, to use the power of compassionate relationships and the influence of mind and body in healing.”
Cristiana Sanna, who attended on behalf of the ANP, said: “Being part of the IMA at this time in history is more important than ever, not only for our members’ benefit but also to ensure the establishment of future partnerships between orthodox medicine and natural therapies.”
Meet the IMA
The Integrated Medicine Alliance (IMA) is a group of organisations that have been brought together for the purpose of encouraging and optimising the best use of natural therapies alongside conventional healthcare for the benefit of all.
The IMA symbolises a new relationship between natural medicine and the health service. We work to encourage integrated patient medical care using conventional and natural health together to optimise health and healing.
Read More
We work closely with social prescribers and conventional healthcare to provide information about how natural therapies may help their patients and how natural therapists can work with conventional healthcare.
The IMA is led by the following principles:
1. A focus on holistic optimal health and healing rather than disease-based models of health.
2. A personalised approach emphasising self-care, personal empowerment and responsibility, respecting the body’s innate healing and transformative potential.
3. A focus on relationship-based care between practitioner and patient.
4. A focus on natural, non-pharmaceutical approaches rather than drug-based therapy, many times using ancient healing wisdom and practices.
5. Decisions informed by evidence and making use of appropriate therapeutic approaches and health care professionals to deliver a personalised approach to health and healing
It is clear that modern medicine, with developments in science and technology, has resulted in a vastly improved understanding, diagnosis, and treatment of disease. Still, this emphasis on science and technology to the exclusion of other elements of healing also limits the development of a holistic and more humane model of healing.
The emphasis on specialist and subspecialist medicine has resulted in an even more fragmented view of holistic person-centred health. At the same time, primary care doctors are overwhelmed by workload and time pressures leaving them insufficient time and resources to address the more holistic aspects of health where they may have insufficient time, training and expertise.
Conventional medical doctors may not be adept at all healing aspects of the human being. Still, they should at least be aware of psychological and spiritual issues in their patients and the implications of ignoring these aspects when it comes to health and healing.
The healing of a patient must include the mental, emotional and spiritual aspects of human health.
The challenge with many natural or holistic practices is that for all their sincere efforts, conventional medical doctors seldom know which of these practices will work with their patients.
Thus, the IMA will aim to help educate, inform, and campaign for these principles.
First Sustainable Healthcare Day – 6th April 2022
Dear ANP member,
This year, on April 6, the ANP and its partners in the Integrated Healthcare Collaborative are supporting the establishment of Sustainable Healthcare Day.
Sustainable Healthcare is one of the most crucial issues facing us as a population. We want you to join us in starting a national conversation about all aspects of this issue and help to raise it up the political agenda.
Read More
We all have a duty to ensure that our healthcare is provided in ways that are sustainable individually, financially, and environmentally. Every one of us is a stakeholder in our health and in that of our planet. We all have a voice and a contribution to make.
In supporting this first Sustainable Healthcare Day, we want the general public, local communities, scientists, businesses, organisations, medical professionals, and politicians to put forward their vision, priorities, and how each can play their part.
We will be asking you to share your stories about how you are contributing to a more sustainable healthcare system. Please share your ideas about where we should focus our efforts. It could be small things you do daily to support your own sustainable individual health, local community projects you run, or greater policy or strategic work that your business or organisation undertakes. The more stakeholders whose voices are heard, the more inclusive and effective our solutions will be.
Sustainable healthcare needs wider publicity and greater action from decision-makers. So on April 6, join the national conversation about how we can take action. Please help us bring this vital issue to the forefront of the healthcare agenda.
Human Rights Act Reform: A consultation on proposals to reform the Human Rights Act 1998
Dear ANP member,
The ANP are writing to bring to your attention the following crucial information. Please take the time to act before the deadline.
Summary:
Human Rights Act Reform: A consultation on proposals to reform the Human Rights Act 1998.
Deadline: 8th March, 11:59hrs.
Web link: https://www.gov.uk/government/consultations/human-rights-act-reform-a-modern-bill-of-rights
Read More
Background:
The UK Government has published a consultation on reforming the Human Rights Act. What exactly does this mean, why should you be concerned and how can you act as a matter of priority to ensure these reforms are not passed?
It is vitally important to understand that Human Rights acts, treaties and legislation do not actually “give people their rights”. These acts, treaties and legislation are meant to guarantee the fact that all human beings already have inherently born, unalienable rights. Therefore, the fact that the UK government is seeking to reform the Human Rights Act, particularly in the context of the current geopolitical picture, is something every UK citizen needs to be concerned about, to scrutinise and to respond to as a matter of priority.
The government portal link above offers a variety of options on how to read and/or download the consultation document and how to respond. Although it is a lengthy document, it is advisable that you read through and understand the ramifications of these reforms, before you fill in and submit your responses. In addition to responding online once you have read the pdf document, you can also email your objections to the proposed reforms here: HRAreform@justice.gov.uk.
You will find a template you can use to base your response on, at the end of this email. You should personalise this response by inserting an introductory paragraph and changing the body of the response to reflect your style, so it does not seem a “bulk template” which may be rejected outright.
Below is a quick view of some of the suggested reforms, with a commentary on their possible implications.
What are the changes about?
The review seeks to impose a rights culture that displaces personal responsibility in favour of “the public interest”. The proposed reforms say, “the international human rights framework recognises that not all rights are absolute and that an individual’s rights may need to be balanced, either against the rights of others or against the wider public interest.” (emphasis added)
Below some further concerning statements:
“The idea that rights come alongside duties and responsibilities is steeped in the UK tradition of liberty, but is also reflected in the qualifications in the Convention and is explicit in Article 29 of the UN Declaration of Human Rights (‘Everyone has duties to the community in which alone the free and full development of his personality is possible’). The increasing reliance on human rights claims over the years has, however, led to a culture of rights decoupled from our responsibilities as citizens, and a displacement of due consideration of the wider public interest”.
“Whilst human rights are universal, a Bill of Rights could require the courts to give greater consideration to the behaviour of claimants and the wider public interest when interpreting and balancing qualified rights. More broadly, our proposals can also set out more clearly the extent to which the behaviour of claimants is a factor that the courts take into account when deciding what sort of remedy, if any, is appropriate. This will ensure that claimants’ responsibilities, and the rights of others, form a part of the process of making a claim based on the violation of a human right”.
“Restrain the ability of the UK courts to use human rights law to impose ‘positive obligations’ onto our public authorities without proper democratic oversight.” (paragraph 229 onwards)
“Make sure that the UK courts are not required to alter or interpret legislation contrary to Parliament’s clearly expressed democratic will.” (paragraph 233 onwards)
There are other concerning statements too, but you get the gist from the above. Both the Executive Summary and the Appendices of the document contain good information to help you, before you read the whole document itself.
Why is it important?
Under the proposed reforms, it appears that Parliament is seeking to impose itself as arbiter of when a person can have human rights and when they cannot. This is extremely concerning. It does not matter the crime, major or minor, a person must always have their human rights protected and available to them. It is abundantly clear that although the proposed reforms mention the courts’ power to decide matters, the government expects the courts to be led on this by parliament, (and legislation), whatever the government decide their rules to be at any given time.
This is an overt attack on personal freedoms in a bid to enforce what amounts to ‘communitarianism’ (which is worse than socialism, and is, in fact, totalitarianism). Wider interests should never trump an individual’s rights, the latter being fundamental, unalienable freedoms.
How to respond?
The proposed reforms indicate that Parliament seeks to become the sovereign power/authority that decides on people’s fundamental rights according to its own agenda, without limits, boundaries and restrictions: precisely what Human Rights protect against.
Giving power to the courts to say you are not entitled to your human rights if they think your behaviour has not been what they consider “good” should be of enormous concern, taking into consideration how reluctant the courts are to challenge government policy decisions. It is important to understand that the proposed changes seek to make sure that Human Rights are NOT fundamental and universal.
The next page offers a template you can customise to your own requirements.
Important note before you continue: Please remember that this concerns your basic, fundamental human rights. So, when you compose your response, think of how you would wish to be treated as a human being. Ask yourself, “What would I want to happen to me if I were in any of the scenarios the reforms are presenting.”
Template email response for personalisation and submission to HRAreform@justice.gov.uk.
To whom it may concern,
I am writing to voice my concerns with regards to the Human Rights Act reform proposal because…. (insert here your own feelings and comments as an introduction – you can use some or all of the points below or, having read the consultation document, form your own. The below is for guidance only).
I want to start by stating that I believe that this reform proposal is entirely unacceptable and I do not support it in any way. I stand for Human Rights and will continue to do so even if the Government tries to take them away through this reform.
The Government should be doing more to uphold Human Rights, yet, I find these proposals weakened and diluted, which is why I cannot and will not support these proposals.
In the nature of the Consultation, I will detail the seven most pressing concerns that I see contained within the Government’s document. This should not be taken as an endorsement of any other part of the reform document, to which I am entirely opposed.
Individual Rights
My first concerns about the Human Rights Act Reform are about how it will impact the individual. I have four main issues that I want to address which are that:
• The proposal of a permission stage will be prohibitive
• The scope of positive obligations will be diminished
• Society could be given more rights than the individual
• An individual’s right to his/her human rights could be judged by the court
The proposal of a permission stage will be prohibitive.
In the reform proposal it proposes that there ought to be a permission stage when an individual wants to bring a Human Rights case before the court. This would ‘require claimants to demonstrate that they have suffered a significant disadvantage before a human rights claim can be heard in court.’ This will have a huge impact upon the number of claimants who are able to bring their case before the courts.
My belief is that our human rights need more protection, not less and bringing in this extra procedural stage with such a high, and undefined, threshold, at the initial stage, before it is even heard in court, means that many human rights abuse cases will go unheard. I do not believe that this is acceptable.
I note the Government has used the same language as European Court of Human Rights protocol 14 but that is a European Court, facing a tremendous backlog. My belief is that as the domestic courts are not facing a backlog and each case referred to the courts will have been committed here in the UK, it ought to be of the highest priority to the UK courts. I also fail to see that it is in any way comparable to the German Federal Constitutional Court which the Government makes reference to.
I want more protection for individuals, not less, therefore, while I stand against the whole notion of this reform I would be particularly concerned about the introduction of a permission stage and believe it would lessen the amount our human rights were upheld.
The scope of positive obligations would be diminished.
There are many people in this nation who are in state-run institutions from hospitals, to care homes, to prisons, to refuges. It has long been established that the state cannot absolve itself of its Human Rights obligations by doing nothing.
If the state does nothing and an individual’s rights are infringed upon and/or abused then the State is responsible, I believe this is rightly so. It is the Government’s obligation to uphold every citizen’s Human Rights.
Yet this proposed reform seeks to pass the buck and put the emphasis on personal responsibility. While I support the notion that we are all responsible for our own conduct, that does not mean the State can ignore Human Rights atrocities happening on its own soil, in its own institutions.
This impact will be felt predominantly by our most vulnerable in society; those with care needs, children in care homes, and so on. I will stand for them and their rights, because they need proactive support. When this is coupled with the previous point which would prevent many of these cases even reaching court it would open up a huge risk of human rights abuses of our most vulnerable.
This, therefore, is another reason that I cannot support these proposals due to the reduction in accountability and increase in the risks that it would cause.
Society could be given more rights than the individual.
We see the Government make mention of ‘wider public interest’ and ‘broader needs of society’ and say that each individual’s needs ought to be balanced against them. While, of course, we all have a duty to conduct ourselves in a way that doesn’t injure or harm another, these definitions are very wide and open to any number of interpretations.
With such wide terms anything that the Government decides could be defined as such could, therefore, be permissible in legislation. This is a very alarming prospect. For example, it could be argued that it is in the broader needs of society for there to be no alcohol as pub brawls and alcoholism are not desirable.
Not only are these proposals concerning upon their own merits, the tone of the Government’s commentary on the matter communicates a distinct disdain for what it calls a ‘rights culture’. Which I can only imagine is, by its definition, when an everyday citizen stands up and demands their Human Rights are respected and officials are held accountable.
I am wholly in favour of an individual being able to do so and I believe it is necessary, as we have lived in a nation that does not uphold Human Rights fully, for far too long. I do not believe an individual’s needs ought to be interfered with for such low and vague criteria and I would not welcome this becoming normalised in our society.
An individual’s rights ought to be cherished and upheld at all times; by doing that it will be of the most benefit to the ‘wider public interest’.
A person’s right to rights could be judged by the court.
Further to the point above, the Government’s derision continues to be evident when it discusses the rights of people whose behaviour it has taken a dislike to.
It states ‘a Bill of Rights could require the courts to give greater consideration to the behaviour of claimants.’ I believe in an individual’s Human Rights and I would not be willing for that to be deemed unnecessary due to past transgressions.
There are no definitions of what ‘behaviour’ would render an individual not worthy of their Human Rights; again, this leaves it wide open for interpretation. Would a missed council tax payment from 15 years prior count? Or discussing a dislike of the Government on social media? This is yet again another very alarming prospect.
Even when an individual has committed a crime that requires a prison sentence, which is clearly an interference with their Human Rights as it is, that does not mean that all their other rights can or ought to then be disregarded.
I am concerned that the Government is essentially stating that you have to earn the right to your rights. This is another part of this reform proposal that I vehemently disagree with, as human rights are unalienable, fundamental rights.
Procedural Matters
Further to the matters that I have outlined above that affect the individual I also have concerns that there are many parts of the reform that will affect the checks and balances at a Parliamentary and judicial level that we rely upon to uphold our human rights. The three main issues that concern me are:
• Judicial amendments will not be allowed unless in line with the will of Parliament.
• Removal of the ability to quash Statutory Instruments.
• Where legislation was once underpinned by the Human Rights Act there is no consideration of the holes left.
Judicial amendments will not be allowed unless in line with the will of Parliament.
We are a nation that prides itself on a Common Law history and we rely heavily upon case law to govern the nation. This has allowed judges to interpret the law and apply it to real world cases and to make judgements without the influence of party politics.
This has been an essential part of the checks and balances that we rely on in this country to protect us from ill-thought-out legislation and undue influence from outside sources.
However, under these proposals the Government will be able to be more prescriptive to the courts giving explicit guidance that they must follow rather than allowing the judges to make interpretations and judgements, essentially preventing a judge from doing their job.
The courts and judges will have to abide by the will of Parliament. Therefore, Parliament will rule all, including the judges and the courts. There will no longer be any separation of power.
I am against the Government giving itself such powers and I believe it could have devastating effects, if not now, in the future, as this would apply to all future Governments.
Removal of the ability to quash Statutory Instruments.
I believe that Statutory Instruments should not be used to make any significant legislation, due to the fact they do not have full consideration of the Houses in the same way that Primary Legislation does. Furthermore, they can be enacted and become law before the House is given any time to debate the matter, if any is even given.
This means Secretaries of State would hold an enormous amount of power as we saw with Matt Hancock and the Health Regulations 2020.
Under the proposals it would prevent courts from being able to overturn any Statutory Instruments that do not uphold people’s Human Rights. This is highly concerning as it means legislation could be passed, quickly and knowingly not in line with Human Rights and there would be no mechanisms to overturn it.
Since 2014 only 14 Statutory Instruments have been overturned but where Statutory Instruments do not have full consideration of the House, and often do not have impact assessments conducted prior to enactment, it is absolutely essential that there is some method to challenge this legislation.
Where legislation was once underpinned by the Human Rights Act it may leave gaping holes.
Currently all legislation passed is underpinned by the Human Rights Act 1998. This means that, where explicit instructions are not contained within the legislation to protect Human Rights, these are implied by the underpinning of the HRA.
The most recent example of this is the Covert Human Intelligence Sources Act. Many members of both Houses fought to have amendments added to the Bill that would have expressly prohibited the use of torture and committing crimes such as rape and murder. However, the Government insisted that it was unnecessary to add them to the Bill as the HRA prohibits them and would underpin the Act.
However, if the Government does away with the Human Rights Act and instead replaces it with a Bill of Rights which states that an individual’s rights can be overridden for ‘broader needs of society’ or if the investigated person’s behaviour is considered lesser than, does that mean a covert human intelligence source can use torture to garner information from them?
The Government gives no consideration or assurances on how it plans to deal with this matter and this means that much legislation could be left with gaping holes in it leading to even more Human Rights abuses with no recourse available to the individual.
These sorts of oversights are highly concerning and do not encourage trust in the Government or its plans of reform.
My belief is that each of the above points is, on an individual basis, abhorrent but all together they combine to make a chilling proposition which I do not believe anyone could be in favour of.
I note that none of the devolved nations have been involved in the construction of this proposed reform and are, in fact, opposed to it. Wales has issued a statement in which they also reference a letter to the Lord Chancellor Dominic Raab, MP, from the Deputy First Minister of Scotland, John Swinney MSP setting out the Scottish Government’s objections too.
Furthermore, in the Welsh statement they reference their own 165-page research paper on the implementation of Human Rights in Wales. The conclusion of that extensive study was that while the Human Rights Act itself is strong and appropriate it needs to be applied more thoroughly so that people’s lived experience reflects it. The conclusion was not to water it down and to take away more individual rights but in actual fact enhance it further.
There was also a lot of evidence gathered by the Independent Human Rights Review in advance of the preparation of the Governments reform proposals and the Government appears to have ignored the majority of it. The evidence affirmed the positive benefits of the Human Rights Act and highlighted, not only the concerns for the people of this nation, but also the potential negative impact around the world if the UK is seen to be regressing in the area of fundamental human rights.
These are our fundamental, unalienable human rights and these are something I believe in. I reiterate my stance that I stand against the notion of a reform from the Human Rights Act to a Bill of Rights in its entirety and believe what the Government should be focusing on is how to uphold our human rights more, not less.
I believe this reform proposal does nothing to serve the individual or society; it merely increases Government control and will, over time, weaken if not entirely erode our fundamental human rights.
This reform must not go ahead.
Yours sincerely
Happy New Year
ANP yearly review, and goals for 2022
As we start the New Year, we wanted to take the time to look back on what we achieved as an association together in 2021 and highlight some of our key goals for 2022.
Dear ANP Member
We hope your new year is getting off to a good start, and you were able to enjoy the holidays with friends and family.
Read More
Our members are the life and soul of our association, and in 2021 we had our best year to date, growing to over 3,000 practitioners.
We look forward to working with you closely in 2022 as we share our passion for natural medicine.
What we achieved in 2021
- Our online Naturopathic Summit was held with 20 keynote speakers and experts in the field of women’s health & hormones.
- The ANP Education Hub was launched to provide additional CPD content and an extensive webinar library for all your education needs.
- Mentoring was a key priority in 2021. We ran 25 different mentoring groups supporting our newly qualified practitioners in their transition to clinical practice.
- We contributed directly to The GNC on behalf of our members, paying their GNC registration fees, so our members didn’t have to pay any additional fees.
- We focused our attention on causes that are important to us, including transparency around covid-19 injections, health freedoms and natural immunity.
- We improved the tech of our website, including implementing automated GNC/ANP membership certificates, and started working with a SEO specialist on driving traffic to our practitioners’ directory profiles
- Our contraindication database was updated with the latest drugs, nutraceuticals and herbs
- We delivered 29 online CPD webinars for our members
What we will be working on in 2022
- Our new mentoring programme will be launched in January. This will include more structured learning for mentees, extra resources, along with better support to help our members be successful in clinical practice
- Implementing the feedback from our 2021 member surveys
- We are moving back to in-person events, both in London and regional areas. Keep an eye out for more events being launched in the next few months.
- Our in-person annual Naturopathic Summit will be on the 24th & 25th of September, 2022. We look forward to sharing our keynote speaker line-up with you soon.
- Our Naturopathy & Community Awards will continue throughout the year, and will feature the hard work of our members as we work to promote them within the community, making naturopathy more well known to the general public.
- We will continue our work with Private Health Insurance companies with the hope to integrate natural therapies into their policies
- We will continue to collaborate with our key partner associations, including the IMA, IHC and GNC, and look to establish a referral system for our members.
- Lastly, while the last few years have left us feeling isolated and out of touch, we are hoping that this year will bring us together, and as such we are looking to do more member outreach and networking so we can understand the needs of our members better, and work together on a united front.
End of Year Survey Results – 2021
Thank you to all of our members who took the time to tell us what they look for and value as part of their ANP membership.
Member feedback helps understand your needs and what is really important to you. As such, this will help drive the direction we take in 2022.
Read More
Let us share the responses:
- 55% of you rate support and advice as the most important feature of what you expect from us here ANP. This was followed by Training & CPD, Networking, Regulation and Legal Support
- Education & CPD was a key response across many questions concerning how ANP can support its members during both their studies and practice. In addition, members highly rated setting up practice support, as well as case studies and business development as a key need for their professional development
- In terms of membership benefits, members value the contraindications database, mentoring programme, discounted insurance, clinic in a box and education as the core benefits they use and value as part of their membership
- Advocacy and career progression was particularly important to many of you, and as such, this will help shape our focus and direction as we work to promote natural medicine to the broader community at large.
- Members also value the information ANP provides through its newsletters and website for the excellent source of information.
- Lastly, we received lots of input from you all on what you would like us to cover for CPD and training purposes. Topics included; covid, gut health and hormones to name a few. Stay tuned to our comms for more information on our new summit, webinars and events!
We look forward to sharing our 2022 plans with you in the coming weeks. Should you have any questions or feedback please reach out on info@theanp.co.uk
World Council For Health – Early COVID-19 Treatment
This is a practical guide for early home treatment of Covid-19.
WCH-At-Home-Treatment-Guide_26-Sept-2021
Top supplements to support female health by BioCare
We often find that many women query how to support their hormones, whether this is for conception, menopause, or due to a specific symptom or condition.
We want you to be able to understand your requirements and help you to pick the right product to meet your own individual needs. Here, we introduce you to some of our most recommended products when it comes to female hormones, fertility, pregnancy, and menopause.
Read More
Multinutrients:
Our multinutrient range is based on high potency, comprehensive and formulations, which contain ingredients in their most easily absorbed form, and with added botanicals for extra antioxidant support.
- Female Multinutrient – for women’s health and hormone balance during childbearing years.
With high levels of biotin, zinc, and vitamins A and C for hair, skin, and nail health, as well as supporting fertility and immunity. It also contains therapeutic levels of B vitamins, including methylcobalamin and methylfolate, and vitamin B6 for hormonal support. As well as all of this, it has the further added benefit of rosemary and green tea extract, for additional antioxidant support, and a gentle, highly absorbable form of iron for energy and cognitive function.
- Methyl Pregnancy Multinutrient – for conception, pregnancy and breastfeeding.
It is our favourite and best multinutrient to support women’s needs from the pre-conceptual stage to nourish the body and support fertility, all the way through pregnancy and breastfeeding. It provides a comprehensive range of nutrients, in particular optimum levels of iron, zinc, lutein, choline and folate. We are using the biologically active form of folate – methylfolate, which is three times more easily absorbed by the body than folic acid, at the recommended dose of 400 micrograms. It also contains lutein, an important antioxidant and pigment, and beta carotene as source of vitamin A.
- Menopause Multinutrient – for women’s health and hormone balance during and after menopause.
Uniquely formulated to support women both peri- and post-menopause, Menopause Multinutrient provides all of the key vitamins and minerals to support a healthy transition. It contains methylcobalamin and methylfolate for added methylation support, vitamins A and C for immune support, green tea extract, lycopene, and higher levels of vitamin E for more targeted hormonal support. It also has higher levels of bone supportive nutrients which are crucial during this time, including vitamins D3 and K2, magnesium, calcium, and boron.
Complexes:
We also have a great range of cleverly formulated complexes, which can be taken alongside a multinutrient, for more personalised, and targeted support.
- Female Balance – botanical complex for women for targeted support.
Female Balance is a clinically effective, potent mix of botanical extracts, specifically designed for women. It includes broccoli sprout as a source of sulphoraphane, red clover, providing a natural source of Isoflavones, as well as beetroot, sage, and green tea extract for antioxidant support, and indole-3-carbinol. Suitable for women during and after childbearing age, and a great addition to a multinutrient.
- Cysteine Complex – botanical, nutrient and antioxidant complex for men and women.
Our classic and highly recommended Cysteine Complex is a specialist combination of amino acids, antioxidants, and plant extracts. It contains broccoli and broccoli sprouts, which are sources of micronutrients and plant chemicals, including sulphoraphanes, glucoraphanins, and indole-3-carbinol, as well as molybdenum, to support sulphite metabolism. In addition to this, it contains N-acetyl cysteine, an amino acid important for the formation of the powerful antioxidant and liver supportive compound, glutathione peroxidase, and pomegranate, a rich source of polyphenols, including ellagic acid. It is a great complex for both men and women, especially if they are exposed to high toxic load, and particularly xenoestrogens – chemicals found in plastics, tap water, cosmetics etc., which can interfere with normal hormone balance.
- P-5-P Complex – nutrient complex for hormone balance
Another favourite, the P-5-P Complex is a combination of vitamin B6 in the form most easily absorbed by the body, pyridoxal-5-phosphate (P-5-P), with cofactors zinc, magnesium and vitamin B2. Vitamin B6 contributes to the regulation of hormonal activity and normal functioning of the nervous system, whilst vitamin B2 can support energy, contributing to the reduction of tiredness and fatigue. Additionally, this product contains a great dose of zinc for the maintenance of healthy hair, skin, and nails. This product can be used on its own to support hormone balance, or in addition to a multinutrient if you require higher dosages of those nutrients.
- Saw Palmetto Complex – for healthy testosterone levels
Saw Palmetto Complex provides a synergistic blend of botanicals, including saw palmetto, with zinc, lycopene, l-arginine, l-carnitine, panax ginseng, and nettle root. Saw palmetto may be particularly useful for men’s health, but can also be used to support women’s health if they need to support their testosterone levels. With added antioxidant support from lycopene, nettle root, and zinc, which contributes to normal fertility, reproduction and the maintenance of normal testosterone levels. A great addition alongside both female multinutrients, depending on your needs.
- Mega GLA Complex – for healthy skin
Our Mega GLA Complex provides a high dose of gamma linolenic acid (GLA), an important omega-6 fatty acid, derived from borage oil (also known as starflower). GLA contributes to the maintenance of the normal structure, elasticity and appearance of the skin. It also contains vitamin E for additional antioxidant support. It provides 180mg of GLA per one capsule. You can take 1 capsule for daily support, or 2-3 if you’d like a higher dose.
We hope this helps to guide your supplement selection, but if you have any questions, or would like some advice based on your specific needs, please contact the Clinical Nutrition team on +44(0)121 433 8702 or clinicalnutrition@biocare.co.uk
Top tips for an easy transition through menopause
“Ageing is not ‘lost youth’ but a new stage of opportunity and strength”
Betty Friedan
Is this how you see menopause? Or are you dreading it? If you are a woman at a perimenopausal age and already thinking about it, or perhaps you are currently going through it and struggling, read on and we’ll delve deeper into how to have an easy transition through menopause and avoid or minimise some of the most common symptoms.
Read More
What happens during menopause?
The menopause is the permanent cessation of menstruation, resulting from the loss of ovarian follicular activity and hence a significant drop in the primary female hormones – oestrogen and progesterone. In the UK, the average age for a woman to reach menopause is 51, although women can experience menopause in their 30s or 40s.[1]Perimenopause is the period that precedes menopause and can start a few years before a woman’s period stops completely. In this phase, hormone levels are gradually starting to decrease and a number of symptoms can start to appear, including irregular menstrual cycles and hot flushes.
Biologically, the ovaries are retiring from their hard work of producing sex hormones. This baton is passed on to the adrenal glands and adipose tissue, which take over the role of hormone production. Due to the widespread activity of oestrogen, menopause is associated with a range of physiological changes such as endothelial dysfunction, oxidative stress, and increased risk of cardiovascular diseases[2] and osteoporosis.[3]
What are the symptoms of menopause?
Our sex hormones regulate so many bodily functions; from circulation, energy production and immunity, to hair or bone growth, which is why menopause often brings on a lot of uncomfortable and debilitating symptoms. Factors such as weight, smoking, alcohol consumption, lack of exercise[4], use of oral contraception[5], history of PMS,[6]and stress[7] can increase risk of menopausal symptoms.
The main symptoms that can occur include:
- Night sweats, hot flushes
- Fatigue
- Weight gain
- Low mood, depression and anxiety
- Digestive discomfort: constipation, bloating, reflux
- Memory and cognitive problems
- Loss of skin elasticity, excessive wrinkling and dryness
- Vaginal dryness and increase in infections such as thrush
The Stress Factor – Are stress and lack of sleep making your menopausal symptoms worse?
As mentioned, once our ovaries stop producing oestrogen, that responsibility goes to our adrenal glands. The adrenal glands also produce our stress hormones – cortisol and adrenaline. High and chronic stress may lead to reduced levels of oestrogen.[8],[9] The stress response also increases body temperature, which may be an additional trigger to hot flushes.[10],[11] Oestrogen also promotes the REM phase of sleep, which is a vital process for healing and repair. When oestrogen levels drop, so does time spent in REM cycles which leads to less refreshing and restorative sleep.[12] Try to reduce your stress levels and promote healthy sleep by increasing magnesium intake[13] and supplementing with relaxing and sleep promoting botanicals such as L-theanine and lemon balm.[14],[15] Turn your bedroom into a sleep sanctuary e.g. dark room, eye mask, technology free.
The Gut Link – Are your gut bacteria responsible for weight-gain during menopause?
Oestrogen is known to have an influence on our gut bacteria, which means that the decrease in oestrogen may contribute to digestive symptoms such as bloating, reflux or constipation during menopause. On the other hand, certain bacteria help to metabolise oestrogen. This gut-hormone interaction has been suggested as an important factor in reducing the risk of oestrogen-dependent cancers.[16] Furthermore, good levels of beneficial bacteria in the genitourinary area is important to prevent vulvovaginal atrophy at menopause, and other complications such as thrush[17] and urinary tract infections.[18] Another exciting role of these bugs is aiding metabolism of fats and carbohydrates as well as insulin levels, hence why poor bacterial balance in the gut can actually increase menopause-associated weight gain. Plant fibre such as inulin[19] promotes healthy digestion and excretion of oestrogen and is effective in promoting weight loss.[20]
Supporting Oestrogen Metabolism
Despite the levels of oestrogen dropping after menopause, it is still important to support healthy breakdown of oestrogen in the body. This is even more important if you are using Hormone Replacement Therapy (HRT). This is because different oestrogen metabolites have different potencies and some of them can be more toxic that others,[21]driving more inflammation, tissue damage and increasing the risk of cancer and cardiovascular disease.
Clinically, we often see that women who struggled with hormonal issues in their reproductive years often have a harder time going through menopause, which may indicate a link with poor oestrogen detoxification, either due to nutritional or genetic causes. A number of nutrients are important to support specific detoxification pathways, namely folate and vitamin B12 for methylation, and Calcium-D-glucarate for glucuronidation, and sulphur for sulphation. Menopausal women are often deficient in folate, B12,[22] as well as zinc and copper.[23]
Furthermore, the sulphur-rich plant chemicals found in cruciferous vegetables (especially broccoli) – sulphoraphaneand indole-3-carbinol.[24],[25],[26] promote healthy detoxification of oestrogen[27],[28],[29] and have been shown to be protective against oestrogen driven cancers (e.g. breast, endometrial and cervical).[30],[31] Also lycopene,naturally found in tomatoes, has been found to reduce the risk of breast and endometrial cancers,[32] and osteoporosis.[33],[34]
The Japanese Paradox
Japanese women are well known around the world for their easy transition through menopause, with far fewer symptoms than women in the Western countries.
One proposed idea is their high intake of plant oestrogens (aka isoflavones), mostly in the form of soya (e.g. tofu, tempeh). These plant molecules structurally resemble body oestrogen but are much less potent, so by increasing your intake through diet, you may fill in the gap of low oestrogen production, and also help with healthy oestrogen metabolism, and even reduce weight gain.[35]
Red clover[36],[37] and sage[38],[39] are also good sources of isoflavones and have been shown to reduce hot flushes, vaginal atrophy, insomnia, cognitive impairment and bone density in menopause.
Interestingly, one paper suggested that the differences in severity of symptoms found in different women around the world may be due to cultural differences in how menopause is perceived and approached.[40] A popular Japanese philosophy called ‘Wabi Sabi’ encourages the acceptance of transience and imperfection; perhaps we need to try to embrace the change and support our body and mind through the transition, rather than fighting and resenting it?
By improving your diet; increasing your vegetable and fibre intake, reducing stress and improving sleep, you can make menopause a much easier transition. If you are however experiencing severe symptoms, a good place to start is a good multivitamin containing methylfolate and methylcobalamin, alongside some isoflavones and extra detoxification support in form of antioxidants and sulphur molecules.
[1] Women’s Health Concern. 2017. The menopause [online] Available at https://www.womens-health-concern.org/help-and-advice/factsheets/menopause/
[2] Lee et al. Independent association between age and natural menopause and hypercholesterolemia, hypertension and diabetes mellitus. Japan Nurses Health Study. J Atheroscler. 2013; 20: 161-9.
[3] Tella SH and Gallagher JC. Prevention and treatment of postmenopausal osteoporosis. J Steroid Biochem Mol Biol. 2014; 142: 155-70
[4] Morris et al. Body Mass Index and other lifestyle factors in relation to age at natural menopause. Am J Epdiemiol 2012 175:998-1105
[5] Pokoradi et al. Factors associated with age of onset and type of menopause in a cohort of UK women. Am J Obstet Gynecol 2011;205:1-13
[6] Freeman et al. Premenstrual Syndrome as a predictor of menopausal symptoms. Obstet Gynecol 2004;103:90-6.
[7] Pimenta et al. Menopausal Symptoms: do life events predict severity of symptoms in peri- and post-menopause? Maturitas 2012, 72:324-31
[8] Gibbs JC et al. The association of a high drive for thinness with energy deficiency and severe menstrual disturbances: confirmation in a large population of exercising women. Int J Sport Nut Exerc Metab. 2011; 21(4): 280-90.
[9] Lasley B et al. Ovarian adrenal interactions during the menopausal transition. Minerva Ginecol. 2013;65(6):641-651.
[10] Gerber LM, Sievert LL, Schwartz JE. Hot flashes and midlife symptoms in relation to levels of salivary cortisol. Maturitas. 2017;96:26–32.
[11] Wods N et al. Cortisol Levels during the Menopausal Transition and Early Postmenopause: Observations from the Seattle Midlife Women’s Health Study. Menopause. 2009;16(4):708-718.
[12] Schwartz and Mong. Estradiol modulates recovery of REM sleep in a time-of-day dependent manner. Am J Physiol Regul Integr Comp Physiol. 2013; 305 (3): R271-280
[13] Park et al. Pilot Phase II trial of magnesium supplements to reduce menopausal hot flashes in breast cancer patients. Support Care Cancer. 2011; 19: 859-63.
[14] Awad R et al. Bioassay-guided fractionation of lemon balm (Melissa officinalis L) using anin vitromeasure of GABA transaminase activity. Phytotherapy Research 2009; 23(8): 1075–8.
[15] Cases J et al. Pilot trial of Melissa officials L leaf in the treatment of volunteers suffering from mild to moderate anxiety disorders and sleep disturbances. Med j Nutrition Metab 2011;4(3):211-218.
[16] Vieira AT, Castelo PM, Ribeiro DA, Ferreira CM. Influence of Oral and Gut Microbiota in the Health of Menopausal Women. Front Microbiol. 2017;8:1884.
[17] Falagas ME, Betsi GI, Athanasiou S. probiotics for the prevention of recurrent vulvovaginal candidaiasis: a review. Journal of Antimicrobial Chemotherapy 2006; 58: 266-272
[18] Karlsson M et al. Substances Released From Probiotic Lactobacillus Rhamnosus GR-1 Potentiate NF-κB Activity in Escherichia Coli-Stimulated Urinary Bladder Cells. Immunol Med Microbiol. 2012 No;66(2):147-56
[19] Van Dokkum et al. Effect of nondigestible oligosaccharides on large-bowel functions, blood lipid concentrations and glucose absorption in young healthy male subjects. Eur J Clin Nutr. 1999; 53 (1): 1-7
[20] Guess et al. A randomized controlled trial: the effect of inulin on weight management and ectopic fat in subjects with prediabetes. Nutrition & Metabolism. 2015 12:36.
[21] Oh H et al. Sitting, physical activity, and serum oestrogen metabolism in postmenopausal women: the Women’s Health Initiative Observational Study. British J of Cancer. 2017;117(7):1070-1078.
[22] Milart et al. Selected vitamins and quality of life in menopausal women. Prz menopauzlny. 2018; 17(4): 175-179
[23] Manafa P et al. Cobalt, Copper, selenium and zinc levels in pre-menopausal and post-menopausal women in Nnewi, South-East Nigeria. Orient J Med. 2015; 27(3-4): 93-98
[24] Park EJ, Pessuto JM. Botanicals in cancer chemoprevention. Cancer Metastasis Rev 2002;21:231-55.
[25] Nestle M. Broccoli sprouts in cancer prevention. Nutr Rev 1998;56:127-30
[26] Zhang Y, Callaway EC. High cellular accumulation of sulphoraphane, a dietary anticarcinogen, is followed by rapid transporter-mediated export as a glutathione conjugate. Biochem J. 2002; 364: 301-7
[27] Li et al. Sulforaphane, a dietary component of broccoli/broccoli sprouts, inhibits breast cancer stem cells. Clinical Cancer Research 2010; 16 (9): 2580–2590.
[28] Conaway CC et al. Disposition of glucosinolates and sulforaphane in humans after ingestion of steamed and fresh broccoli. Nutr Cancer 2000;38:168-78.
[29] Michnovicz et al. Changes in levels of urinary estrogen metabolites after oral indole-3-carbinol treatment in humans. J Natl Cancer Inst 1997;89(10):718-23.
[30] Auborn et al. Indole-3-carbinol is a negative regulator of estrogen. J Nutr. 2003;133(7 Suppl):2470S-2475S
[31] Kunimasa et al. Indole-3-carbinol Suppresses Tumor-Induced Angiogenesis by Inhibiting Tube Formation and Inducing Apoptosis. Biosci Biotechnol Biochem. 2008;72(8):2243-6.
[32] Nahum A. et al. Lycopene inhibition of cell cycle progression in breast and endometrial cancer cells is associated with reduction in cyclin D levels and retention of p27kip1 in the cyclin E-cdk2 complexes. Oncogene. 2001; 20: 3428-3436
[33] Mackinnon ES et al. Supplementation with the Antioxidant Lycopene significantly decreases oxidative stress paramenters and the bone resorption marker N-telopeptide of Type 1 Collagen in Postmenopausal women. Osteoporosis Int. 2011; 22(4): 1091-101
[34] Ardawi MM et al. Lycopene Treatment against Loss of Bone Mass, microarchitecture and strength in relation to regulatory mechanisms in a postmenopausal Osteoporosis model. Bone. 2016; 83: 127-140
[35] Vieira AT, Castelo PM, Ribeiro DA, Ferreira CM. Influence of Oral and Gut Microbiota in the Health of Menopausal Women. Front Microbiol. 2017;8:1884.
[36] Bedell. The pros and cons of plant oestrogens for menopause. J Steroid Biochem Mol Biol 2012,epub Dec 25
[37] Guttuso. Effect and clinically meaningful non-hormonal hot flash therapies. Maturitas 2012, 72;6-12
[38] Bommer S, Klein P and Suter A. First time proof of Sage’s Tolerability and Efficacy in Menopausal Women with hot flushes. Adv Ther. 2011; 28(6): 490-500
[39] Forouhari S et al. The effect of salvia officinalis tablet on hot flashes, night sweating and estradiol hormone in postmenopausal women. Int J Med Res Health Sci. 2016; 5(8): 257-263
[40] Center For The Advancement Of Health. “Menopause Affects Japanese Women Less Than Westerners.” ScienceDaily. ScienceDaily, 27 July 1998.
Endometriosis – The Common, Yet Under-Diagnosed Condition
by Raihane Palagi
The average woman can spend 10 years, or 3650 days, having a period. For many, these are years of life-affecting symptoms, such as debilitating pain and fatigue. This is especially the case for women with endometriosis. One in ten women in the UK have endometriosis, but diagnosis is tricky and can take up to a staggering 7.5 years.[i]
Read More
Endometriosis is the growth of cells from the uterine lining, the endometrium, in other areas such as the ovaries or colon. These cells respond to hormone fluctuations in the same way as in the uterus, thickening under the influence of oestrogen and then shedding after the sudden drop of progesterone, in absence of fertilisation. However, unlike the cells in the uterus, these cells have nowhere to escape, making menstruations extremely painful and causing a whole lot of symptoms.
Key Symptoms:
Hormonal fluctuations are part of a normal female monthly cycle, so experiencing mild abdominal cramps and breast tenderness, can be normal for some individuals. For endometriosis, other symptoms can include:
- Painful and heavy periods
- Infertility
- Back, pelvic, and ovulation pain
- Painful bowel movements, urination, and intercourse
- Bleeding between periods
- Nausea
- Extreme tiredness
What Are the Main Drivers?
Retrograde menstruation, when menstrual blood containing endometrial cells flows back through the fallopian tubes, has long been deemed as the main cause of endometriosis.[ii],[iii] However, more recent research highlights many other compounding factors.
Oestrogen dominance, is often debated when discussing endometriosis.[iv] Oestrogen is one of the main hormones that regulates the menstrual cycle. It drives the development of the reproductive tract and thickens the endometrium to prepare the uterus for the ovulation and egg implantation. This stems from the ability of oestrogen to promote cell proliferation. However, if oestrogenic activity becomes enhanced, it can drive excessive cell proliferation, possibly contributing to endometriosis.
This can happen when oestrogen synthesis is stimulated by factors such as excessive carbohydrate intake,[v] being overweight,[vi] stress,[vii] and working night-shifts.[viii] Shift work has been associated with a 50% increased risk of endometriosis.[ix] Oestrogenic activity can also be heightened by exposure to environmental chemicals which mimic its activity, for example xenoestrogens from plastics.[x],[xi]
Oestrogen is kept within balance thanks to complex detoxification processes performed by your body, mainly methylation, glucuronidation, and sulphation. Unfortunately, many women have a reduced ability to perform these processes and effectively metabolise and eliminate oestrogen. This is exacerbated by high intake of paracetamol[xii] and smoking,[xiii] coupled with low intake of cruciferous vegetables,[xiv] folate, B12,[xv] and magnesium.[xvi],[xvii] Disrupted methylation, in particular, has been directly linked with endometriosis.[xviii]
Gut health can also play a role. Under normal circumstances, oestrogen metabolites are shunted from the liver into the gut in bile and eliminated through daily bowel movements. Dysbiosis, constipation, and intestinal permeability (‘Leaky Gut’), can increase the risk of oestrogen metabolites being re-absorbed, rather than eliminated, and so, oestrogen dominance. Women with endometriosis can also be prone to irritable bowel syndrome (IBS),[xix] highlighting the gut-hormone connection.
Elevated inflammation has been identified during, and as a driver of, endometriosis.[xx] Excess weight,[xxi] disrupted sleep,[xxii] processed food,[xxiii] low omega-3 intake,[xxiv] and stress,[xxv] can further increase inflammation and may worsen symptoms. Wider immune dysfunction also seems to be involved. Antibodies targeting our own cells have been identified in extra-uterine endometrial tissue,[xxvi] indicating an autoimmune component to this condition.[xxvii] Low vitamin D is a risk factor for autoimmunity,[xxviii] and interestingly, increases endometriosis risk.[xxix]
What Can You Do?
- If overweight, implement sustainable weight loss. Consider daily exercise, reduced carbohydrate intake, and increased intake of nutrients to support blood glucose regulation, such as [xxx]
- Enjoy daily relaxation and increase intake of calming nutrients, such as magnesium.[xxxi]
- Reduce xenoestrogen exposure by minimising plastic use and switching to natural cosmetics.
- Increase phytoestrogen intake from red clover and flaxseeds, which weakly bind to oestrogen receptors, blocking more stimulating oestrogens.[xxxii],[xxxiii]
- Support oestrogen detoxification by increasing intake of sulphoraphane,[xxxiv] N-acetyl cysteine,[xxxv] and glucobrassicin through dietary sources, such as cruciferous vegetables, or supplementation.
- Quit smoking and reduce intake of smoked/charred and non-organic food, caffeine, and alcohol to further take pressure off the liver.
- Test for nutrient deficiencies such as folate, B12, B6, iron, and vitamin D via the GP or privately.
- Increase omega-3 intake though oily fish, hemp and flaxseeds to reduce inflammation and endometriosis risk.[xxxvi]
[i] Diagnostic survey form Endometriosis UK https://www.endometriosis-uk.org/endometriosis-facts-and-figures#5
[ii] Sampson JA. Metastatic or embolic endometriosis, due to the menstrual dissemination of endometrial tissue into the venous circulation. Am J Pathol.1927;93:110–43.
[iii] D’Hooghe, T, Debrock, S. Endometriosis, retrograde menstruation and peritoneal inflammation in women and in baboons. Human Reproduction Update. 2002; 8 (1): 84-88.
[iv] Vercellini P et al. Endometriosis: pathogenesis and treatment. Nat Rev Endocrinol. 2014; 10(5): 261-75
[v] Fulghesu AM et al. The impact of insulin secretion on the ovarian response to exogenous gonadotropins in polycystic ovary syndrome. J Clin Endocrinol Metab. 1997; 82 (2): 644-8.
[vi] Williams G. Aromatase up-regulation, insulin and raised intracellular oestrogens in men, induce adiposity, metabolic syndrome and prostate disease, via aberrant ER-α and GPER signalling. Mol Cell Endocrinol. 2012;351(2):269-78
[vii] McTernan PG et al. Gender differences in the regulation of P450 aromatase expression and activity in human adipose tissue. International Journal of Obesity. 2000; 24:875-881
[viii] Nagata C et al. Light exposure at night, urinary 6-sulfatoxymelatonin and serum estrogens and androgens in postmenopausal Japanese women. Cancer Epidemiol Bio Prev. 2008; 17 (6).
[ix] Marino JL et al. Shift work, hCLOCK T3111C polymorphism and endometriosis risk. Epidemiology.2008;19(3):477-84.
[x] Darbre PD, Harvey PW. Parabens can enable hallmarks and characteristics of cancer in human breast epithelial cells: a review of the literature with reference to new exposure data and regulatory status. J Appl Toxicol. 2014;34:925–38.
[xi] Krishnan AV et al. Bisphenol-A: an estrogenic substance is released from polycarbonate flasks during autoclaving. Endocrinology. 1993;132:2279–86.
[xii] Gill et al. MicroRNA regulation of CYP 1A2, CYP3A4 and CYP2E1 expression in acetaminophen toxicity. Sci Rep. 2017; 7: 12331.
[xiii] Shimada T, Fujii-Kuriyama Y. Metabolic activation of polycyclic aromatic hydrocarbons to carcinogens by cytochromes P450 1A1 and 1B1. Cancer Sci. 2004; 95 (1): 1-6.
[xiv] Michnovicz et al. Changes in levels of urinary estrogen metabolites after oral indole-3-carbinol treatment in humans. J Natl Cancer Inst 1997;89(10):718-23.
[xv] Herrmann W et al. Vitamin B-12 status, particularly holotranscobalamin II and methylmalonic acid concentrations, and hyperhomocysteinemia in vegetarians. Am J Clin Nutr. 2003;78(1):131-6.
[xvi] Tsao D et al. Structural mechanisms of S-adenosyl methionine binding to catechol O-methyltransferase. PLoS One. 2011; 6 (8): e24287
[xvii] Dawling S et al. Catechol-O-methyltransferase (COMT)-mediated metabolism of catechol estrogens: comparison of wild-type and variant COMT isoforms. Cancer Res. 2001;15;61(18):6716-22.
[xviii] Ji F et al. Aberrant endometrial DNA methylome of homeobox A10 and catechol-O-methyltransferase in endometriosis. J Assist Reprod Genet. 2017;34(3):409-415.
[xix] Seaman et al. Endometriosis and its coexistence with irritable bowel syndrome and pelvic inflammatory disease: findings from a national case-control study. BJOG. 2008 Oct;115(11):1392-6.
[xx] Meng-Hsing W et al. Endometriosis and possible inflammation markers. Gynecology and Minimally Invasive Therapy. 2015; 4 (3): 61-67.
[xxi] Coppack SW. Pro-inflammatory cytokines and adipose tissue. Proc Nutr Soc. 2001;60(3):349-56. Review.
[xxii] Morris et al. Sleep Quality and Duration are Associated with Higher Levels of In ammatory Biomarkers: the META-Health Study. Circulation. 2010; 122: A17806.
[xxiii] Erridge C. The capacity of foodstuffs to induce innate immune activation of human monocytes in vitro is dependent on food content of stimulants of Toll-like receptors 2 and 4. Br J Nutr. 2011;105 (1): 15-23.
[xxiv] Bokor S et al. Single nucleotide polymorphisms in the FADS gene cluster are associated with delta-5 and delta-6 desaturase activities estimated by serum fatty acid ratios. J Lipid Res. 2010; 51 (8): 2325-2333.
[xxv] Gouin. Chronic Stress, Immune Dysregulation, and Health. Am J Life Med. 2011; 5: 476-85.
[xxvi] Zhang et al. The link between immunity, autoimmunity and endometriosis: a literature update. Autoimmunity Reviews 17 (2018) 945–955
[xxvii] Olof et al. Risk of endometriosis in 11 000 women with celiac disease. Human Reproduction, Vol.26, No.10 pp. 2896–2901, 2011
[xxviii] Simpson et al. Latitude is significantly associated with the prevalence of multiple sclerosis: a meta-analysis. J Neurol Neurosurg Psychiatry. 2011; 82 (10): 1132-41.
[xxix] Ciavattani et al. Ovarian endometriosis and vitamin D serum levels. Gynecological Endocrinology Volume 33, 2017 – Issue 2
[xxx] Martin et al. Chromium picolinate supplementation attenuates body weight gain and increases insulin sensitivity in subjects with type 2 diabetes. Diabetes Care. 2006 Aug; 29(8): 1826-32.
[xxxi] Held K et al. Oral Mg supplementation reverse age-related neuroendocrine and sleep EEG changes in humans. Pharmacopsychiatry 2002; 35(4):135-43.
[xxxii] Cassidy. Potential tissue selectivity of dietary phytooestrogens and oestrogens. Curr Opin Lipidol 1999;10:47-52.
[xxxiii] Brzezinski et al. Phytooestrogens: the “natural” selective oestrogen receptor modulators? Eur J Obstet Gynecol 1999;85:47-51.
[xxxiv] Heiss E, Herhaus C, Klimo K, et al. Nuclear factor kappa B is a molecular target for sulforaphane-mediated anti-inflammatory mechanisms. J Biol Chem 2001;276:32008-15.
[xxxv] Porpora et al. A promise in the treatment of endometriosis: an observational cohort study on ovarian endometrioma reduction by N-acetylcysteine Evidence-based complementary and alternative medicine : eCAM vol. 2013: 240702.
[xxxvi] Stacey et al. A prospective study of dietary fat consumption and endometriosis risk. Hum Reprod. 2010 Jun; 25(6): 1528–1535.
The thyroid and PMS link: overt and subclinical conditions
By Samuel Peters BHSc Nat
Thyroid indices have been reported to be more variable in women with PMS compared with healthy controls.1-3 Some studies indicate that the absolute levels of thyroid hormones are not altered, but that their timing of excretion may be dysfunctional.1,4 Regardless, both overt and subclinical hypothyroidism are known to cause numerous disturbances to the menstrual cycle and disrupt hormonal homeostasis.5,3 The prevalence of subclinical hypothyroidism, defined as raised TSH with normal serum T4 and T3 concentrations is reported to be two times higher in women with menstrual disorders compared to healthy controls.3
Read More
The molecular link between thyroid dysfunction and disturbances in ovarian hormone synthesis and ovulation is still largely unknown. Hypothyroidism results in decreased metabolic clearance of androstenedione and oestrone and increases peripheral aromatisation. Plasma binding activity of sex hormone-binding globulin (SHBG) is also decreased, resulting in increased concentration of unbound testosterone and oestradiol. Disorders of the thyroid also precede dysregulation of the hypothalamic-pituitary-gonadal axis and is often associated with oligomenorrhea.6
As peripheral thyroid hormones readily cross the blood brain barrier, disruptions to thyroid hormones are also expected to have an effect on mood, cognition and emotional processing. Low T4 concentration and an increased T3/T4 ratio has been found to be associated with an increase in PMS symptom severity.7
Essential prescribing approaches
Per gram, thyroid tissue contains the highest concentration of selenium in the body due to the abundant expression of selenoproteins including glutathione peroxidase, thioredoxin reductases and deiodinases. These enzymes function in redox homeostasis and in thyroid hormone synthesis and metabolism.8 Many farming areas in Australia have poor soil selenium content which may be further depleted by farming practices, and several studies have indicated that selenium levels have declined by approximately 20% in the Australian population since the 1970’s.9
Iodine is essential for thyroid hormone synthesis and intake has also declined in Australia, most likely due to public health recommendations to reduce salt intake together with the reduction of iodine content of dairy products.10
Supplementation of these key thyroid supporting nutrients may be an important therapeutic considerations for women experiencing symptoms of PMS with suboptimal thyroid function.
References:
- Girdler, S. S., Pedersen, C. A., & Light, K. C. (1995). Thyroid axis function during the menstrual cycle in women with premenstrual syndrome. Psychoneuroendocrinology, 20(4), 395–403.
- Schmidt, P. J., Grover, G. N., Roy-Byrne, P. P., & Rubinow, D. R. (1993). Thyroid function in women with premenstrual syndrome. The Journal of Clinical Endocrinology & Metabolism, 76(3), 671–674. http://doi.org/10.1210/jcem.76.3.8445024
- Ajmani, N. S., Sarbhai, V., Yadav, N., Paul, M., Ahmad, A., & Ajmani, A. K. (2016). Role of Thyroid Dysfunction in Patients with Menstrual Disorders in Tertiary Care Center of Walled City of Delhi. The Journal of Obstetrics and Gynecology of India, 66(2), 115–119. http://doi.org/10.1007/s13224-014-0650-0
- Yonkers, K. A., O’Brien, P. M. S., & Eriksson, E. (2008). Premenstrual syndrome. Lancet (London, England), 371(9619), 1200–10. http://doi.org/10.1016/S0140-6736(08)60527-9
- Krassas, G. E., Poppe, K., & Glinoer, D. (2010). Thyroid Function and Human Reproductive Health. Endocrine Reviews, 31(5), 702–755. http://doi.org/10.1210/er.2009-0041
- Saran, S., Gupta, B. S., Philip, R., Singh, K. S., Bende, S. A., Agroiya, P., & Agrawal, P. (2016). Effect of hypothyroidism on female reproductive hormones. Indian Journal of Endocrinology and Metabolism, 20(1), 108–13. http://doi.org/10.4103/2230-8210.172245
- Bunevicius, A., Leserman, J., & Girdler, S. S. (2012). Hypothalamic-pituitary-thyroid axis function in women with a menstrually related mood disorder: association with histories of sexual abuse. Psychosomatic Medicine, 74(8), 810–6. http://doi.org/10.1097/PSY.0b013e31826c3397
- Drutel, A., Archambeaud, F., & Caron, P. (2013). Selenium and the thyroid gland: more good news for clinicians. Clinical Endocrinology, 78(2), 155–164. http://doi.org/10.1111/cen.12066
- Lyons, G. H., Judson, G. J., Stangoulis, J. C. R., Palmer, L. T., Jones, J. A., & Graham, R. D. (2004). Trends in selenium status of South Australians. The Medical Journal of Australia, 180(8), 383–6.
- Thomson, C. D. (2004). Selenium and iodine intakes and status in New Zealand and Australia. British Journal of Nutrition, 91(5), 661. http://doi.org/10.1079/BJN20041110

Clinical Approaches to Oestrogen Deficiency
By Samuel Peters BHSc Nat
Oestrogen is traditionally thought of as a product of the ovaries, however it is also able to be synthesised in areas such as the placenta, skin, adipose tissue and even the brain, which can contribute significantly to the local and circulating pool of oestrogens. Aromatase is the key enzyme that regulates oestrogen production in the peripheral tissues, catalysing the conversion of steroid precursors (androgens) to oestrogens.1,2
Oestradiol is the most active form of oestrogen, and is able to be converted to oestrone and back to oestradiol depending on physiological requirements. Either form can then be converted to oestriol, the major urinary metabolite. Oestrogens circulate in the body, bound primarily to sex-hormone binding globulin (SHBG), however only free oestrogen is available to exert biological activity and enter target tissues.1,2
Read More
Oestrogen excess
A state of oestrogen excess may result from increased oestrogen production or result from inadequate clearance via the liver or bowels. A state of relative oestrogen excess may also occur when oestrogen levels are normal but progesterone synthesis is low and oestrogen is ‘unopposed’. There may also be impaired inactivation from the more active oestradiol to oestrone.1
Implications in PMS
The variety of PMS subtypes are thought to be related to hormonal fluctuations which vary from individual to individual.
PMS subtype-A (anxiety) is thought to be related to high levels of oestrogen and a deficiency of progesterone. PMS-D (depression) is thought to be related to low oestrogen levels resulting in excessive breakdown of neurotransmitters. PMS-H (hyperhydration) is thought to be due in part to oestrogen induced elevations in aldosterone.3
The regulation of upstream signalling hormones should be the first consideration for clinicians, as the hypothalamic-pituitary-ovarian (HPO) axis is the master regulator of the balance between oestrogen and progesterone synthesis. As HPO regulating botanical, Chaste Tree is indicated for numerous gynaecological conditions, including PMS (except possibly PMS-C (carbohydrate craving)).4
Aromatase inhibitors are important considerations in conditions of oestrogen excess. Grape seed extract has demonstrated significant aromatase inhibition both in vitro and in vivo.5 Zinc is also known to inhibit aromatase activity.6
Oestrogen detoxification
Detoxification of hormones plays a key role in the treatment approach for a number of gynaecological conditions including PMS.7
Oestrogen excretion via the liver occurs primarily though phase I hydroxylation and the phase II pathways, methylation, glucuronidation and sulfation. Supporting herbs and nutrients are outlined in the table below.
| Supporting herbs and nutrients for oestrogen detoxification8 | ||
| Pathway | Supporting nutrients | Induced by |
| Phase I | ||
| Hydroxylation | B2, B3, B6, B9, B12, Glutathione |
Caffeine High protein diet Flavonoids Rosemary |
| Phase II | ||
| Methylation | Folate, B2, B6, B12, DMG, Mg |
Dandelion Milk Thistle Withania Curcumin NAC Green tea Caffeine Garlic Bioflavanoids |
| Glucuronidation | Taurine | |
| Sulfation | Methionine, Cysteine, NAC, Glutathione | |
Physical activity in conjunction with a high fibre diet is also thought to promote elimination of hormones via the bowel. Hormones excreted via the bile may be reabsorbed into enterohepatic circulation when bowel transit time is slow.8
If you would like to learn more about practitioner only products that support oestrogen detoxification then visit www.biomedica.uk.com or contact local BioMedica representative Lucy Peel lucy@biomedica.uk.com
BioMedica products are available to be ordered via https://naturaldispensary.co.uk/ and https://www.amritanutrition.co.uk/
References:
- Bulun, S. E., Gurates, B., Fang, Z., Tamura, M., Sebastian, S., Zhou, J., … Yang, S. (2002). Mechanisms of excessive estrogen formation in endometriosis. Journal of Reproductive Immunology, 55(1–2), 21–33.
- Nelson, L. R., & Bulun, S. E. (2001). Estrogen production and action. Journal of the American Academy of Dermatology, 45(3 Suppl), S116-24.
- Wardle, J. (2014). Dysmenorrhoea and menstrual complaints. In J. Sarris & J. Wardle (Eds.), Clinical Naturopathy (2nd ed., pp. 423–438). Sydney: Elsevier.
- Bone, K., & Mills, S. (2013). Principles and Practice of Phytotherapy (2nd ed.). Churchhill Livingstone.
- Balunas, M. J., Su, B., Brueggemeier, R. W., & Kinghorn, A. D. (2008). Natural products as aromatase inhibitors. Anti-Cancer Agents in Medicinal Chemistry, 8(6), 646–82.
- Askary, V. R., Jahan, N. A., Sabbagh, A., Jahani, F. S., Dourandish, N., & Kamachali, A. R. K. (2011). A potential medicinal importance of zinc in human health and chronic diseases. Clinical Biochemistry, 44(13), S323–S324. http://doi.org/10.1016/j.clinbiochem.2011.08.795
- Wardle, J. (2014). Endometriosis. In J. Sarris & J. Wardle (Eds.), Clinical Naturopathy (2nd ed., pp. 440–451). Sydney: Elsevier.
- Salmond, S. (2014). Liver Dysfunction and Disease. In J. Sarris & J. Wardle (Eds.), Clinical Naturopathy (2nd ed., pp. 131–158). Sydney: Elsevier.
PMS and the stress connection
By Samuel Peters BHSc Nat
Chronic stress is associated with altered HPA axis function in women with PMS and several studies have also reported that stress levels are associated with PMS symptom severity. In multiple studies, women with PMS have failed to demonstrate activation of the HPA axis following stressful stimuli. Whilst controls saw an increase in luteal phase vasopressin (AVP), adrenocorticotrophic hormone (ACTH) and cortisol in response to exercise induced stress, women with PMS failed to demonstrate this normal physiological response, suggesting that dysregulation of the stress response plays a role in PMS pathophysiology.1 Furthermore, the degree of hyporeactivity of the HPA axis appears to predict PMS symptom severity.2
Read More
A recent longitudinal study assessed the association between psychosocial stress in the previous month and the risk of subsequent perimenstrual symptoms. It was found that high perceived stress was strongly associated with a significantly increased risk of experiencing multiple moderate/severe PMS symptoms in the subsequent cycle. High perceived stress was associated with an 8 fold increase risk of reporting ≥8 moderate/severe perimenstrual symptoms, and a 2.66 fold increased risk of reporting ≥5 moderate/severe perimenstrual symptoms. For women whose stress levels increased or decreased from cycle 1 to cycle 2, their symptom severity patterns appeared to follow their stress levels. Furthermore, in women who reported low stress levels preceding both cycles compared to those reporting high stress levels preceding both cycles, the occurrence of ≥8 moderate/severe symptoms was 25 times lower.3
Slight irregularities in the normal variation of ovarian hormones throughout the menstrual cycle is one of many proposed underlying pathological factors in PMS, however consistent patterns are yet to be identified. Psychosocial stress is thought to impact the severity of premenstrual symptoms by altering ovarian hormone levels.3 The neuromodulatory effects of gonadal steroids are well appreciated and also believed to play a role in PMS.4 Perceived stress may directly or indirectly lead to altered levels of neurotransmitters and other cognitive processes.3
Stress management is a primary naturopathic treatment aim in women with PMS, encompassing herbal, nutritional and lifestyle interventions.
| Therapeutic tools for stress management in women with PMS | |
| Herbal |
Saffron Withania Siberian ginseng Rhodiola Rehamnnia Lavender Skullcap |
| Nutritional |
B Complex vitamins Tyrosine Vitamin C Magnesium Zinc |
| Lifestyle |
Work/life balance and self-care strategies. Meditation Exercise Yoga Breathing exercises Counselling |
References:
- Roca, C. A., Schmidt, P. J., Altemus, M., Deuster, P., Danaceau, M. A., Putnam, K., & Rubinow, D. R. (2003). Differential menstrual cycle regulation of hypothalamic-pituitary-adrenal axis in women with premenstrual syndrome and controls. Journal of Clinical Endocrinology and Metabolism, 88(7), 3057–3063. https://doi.org/10.1210/jc.2002-021570
- Huang, Y., Zhou, R., Wu, M., Wang, Q., & Zhao, Y. (2015). Premenstrual syndrome is associated with blunted cortisol reactivity to the TSST. Stress, 18(2), 160–168. https://doi.org/10.3109/10253890.2014.999234
- Gollenberg, A. L., Hediger, M. L., Mumford, S. L., Whitcomb, B. W., Hovey, K. M., Wactawski-Wende, J., & Schisterman, E. F. (2010). Perceived stress and severity of perimenstrual symptoms: the BioCycle Study. Journal of Women’s Health (2002), 19(5), 959–967. https://doi.org/10.1089/jwh.2009.1717
- Ribinow, D., & Schmidt, P. (2006). Gonadal steroid regulation of mood: The lessons of premenstrual syndrome☆. Frontiers in Neuroendocrinology, 27(2), 210–216. https://doi.org/10.1016/j.yfrne.2006.02.003
A Naturopathic Iridology Case
By Elle Fox, Snr Editor, ANP
A naturopathic iridology assessment (analysis of the eye’s iris) can be very successfully used as part of the naturopathic consultation in order to reveal a person’s underlying constitution and support the development of an individual naturopathic treatment protocol, as the following case demonstrates.
Read More
The patient is a fair, slim, athletic female of 45yrs presenting with:
- Chronic low blood sugar resulting in migraines (kaleidoscope) ‘seeing stars’; since early 20s
- Formication (crawling under the skin); last 6yrs
- Loose bowels pm (painless but preceded by mild nausea)
The patient came for a naturopathic iridology assessment because she felt that the medical tests and treatment she had undertaken over the years had not resolved her health problems.
Medical History:
Childhood: patient had received all childhood vaccinations; was hospitalised “after a shot” but had no more information available.
Adulthood: “niggly health problems” as above.
Drug history: OCP in 20s; ex-smoker; occasional antibiotics prescribed for odd chest or skin infections; Cetirizine last 6yrs regularly; up to date boosters (DTP) plus travel inoculations 6yrs ago, incl. yellow fever vaccine. Patient felt very unwell after this, with nausea, vomiting and developing a skin rash. Was treated with topical steroid cream.
Surgery/hospitalisation/dental: had 4 molars taken out 6yrs ago under sedation and prophylactic antibiotics after the procedure. Patient reports that she started experiencing “crawling under skin” whilst she was taking the antibiotics. The dental extraction was performed 5 weeks after the yellow fever vaccine reaction.
Other information: patient had lost her mother 6 years previously and still felt the loss (the loss of the parent happened a few months prior to the dental procedure).
Mainstream Treatment to date:
No medical treatment for hypoglycaemia; migraine medication had been offered which the patient did not wish to take.
Medical investigation for allergies was inconclusive. Patient thinks she is premenopausal but blood tests did not show any hormone imbalances (formication can be a symptom of lower oestrogen). Test for scabies was negative. Allergy tablets containing Cetirizine were prescribed; patient has been taking these every 48 hrs for 6 yrs to manage formication symptoms as well as her allergic reactions to animal danders and hay fever symptoms. The list of the common adverse effects of Cetirizine from NHS website includes diarrhoea and nausea; the patient reports these issues with her health.
Current system status:
Regular bouts of low blood sugar and associated migraines
Sleeps 6-8hrs, wakes unrefreshed
Feels congested (sinuses, sluggishness)
Allergies to animal danders, early pollens and summer grasses
Bloating after eating certain foods, esp. sugars, grains
Regular menses with mild PMT; libido variable to low
No pregnancies
Patient reports good appetite, eats organic food, exercises regularly, (competitive dressage), lives in the countryside
Thirstless but drinks water with lemon first thing am and during the day
2 coffees in the morning
Glass of red wine most evenings
Recently embraced fermented foods – warned about histamine effects so experimenting with careful introduction.
Sports: Running, yoga, competitive riding/dressage, gardening
Overall level of satisfaction in life 6 out of 10
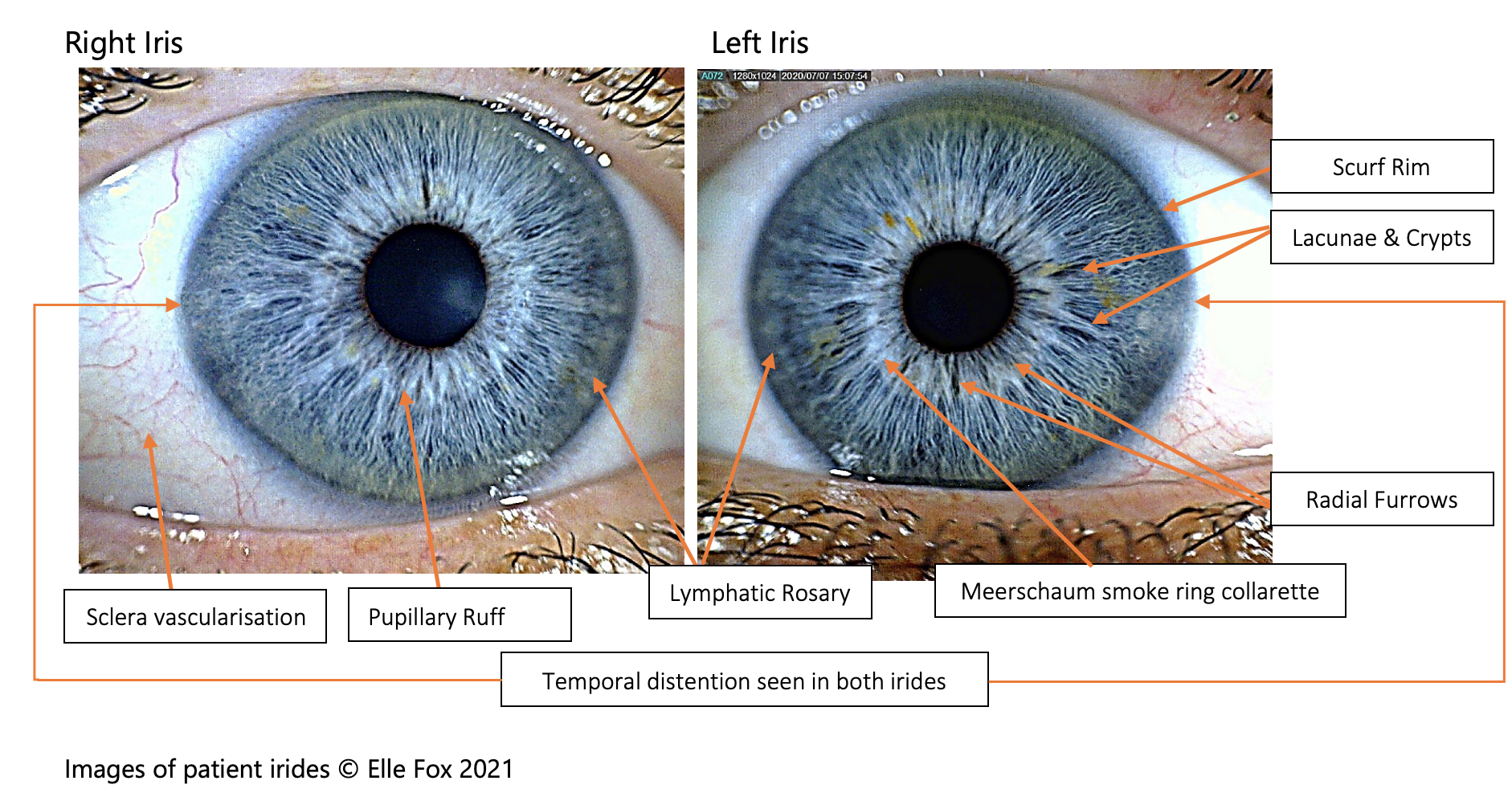
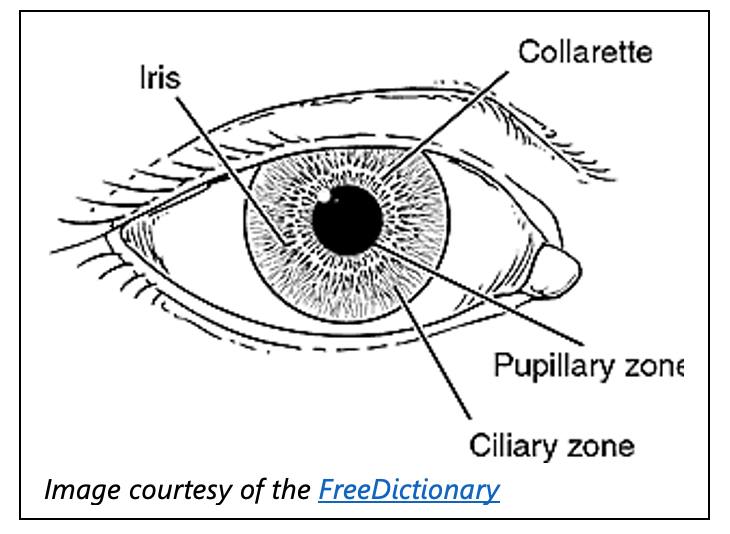 Iris Markings and Observations*
Iris Markings and Observations*
- This is a high-resistance, robust iris and its owner finds it difficult to relax. The iris fibres have a combed hair appearance with distinctive radial furrows, conspicuous crypts and very few defined lacunae (dark, leaf-shaped areas).
- Irritation fibres and a lymphatic rosary are noticeable as is a pale yellow overlay at the outer ciliary zone pointing to hyperacidity and chronic inflammation.
- The irides have a ‘Meerschaum smoke ring’ collarette which points to high levels of catarrh and acidity.
- Radial furrows at the pupil margin point to increased risk of gut ulceration.
- A prominent scurf rim denotes difficult elimination through the skin.
- Fine vascularisation of the sclera is pointing to increased reactivity (allergic diathesis).
- Pancreotropic pigment markings and other iris markings indicate blood sugar dysregulation as do the temporal distensions (both irides bulge out at the outer side) in both irides which indicate possible lack of vitamin B3 (blood sugar regulation disturbance); this strengthens the likelihood of pancreatic involvement.
- Reddish brown noticeable pupillary ruff points to a possibility of stomach lining inflammation.
The iris map[i] corresponds with specific areas of the body; depending on where particular markings on the patient irides are in relation to the organ/s, the practitioner may include in the treatment programme specific support for that or those organs correspondingly.
(*) This is a very broad summary. There is a much more detailed chart of iris markings and associated comments available on request.
Treatment Plan Recommendations
Further testing:
Since the patient refused to have additional medical testing done via her GP surgery (“been there, done that”), she was recommended a simple, non-invasive urine organic acids test (OAT). It was explained to the patient that the OAT can identify issues related to metabolic dysfunction and toxic compound build-up in the body which may upset glucose, amino acid and fat metabolism and cause ‘acidaemias’. Some of these acidaemias, particularly those that involve the oxidation of fatty acids, can cause intermittent hypoglycaemia[ii]. OAT tests can indicate these acidaemias as well as the presence of yeast and bacteria metabolites[iii]:
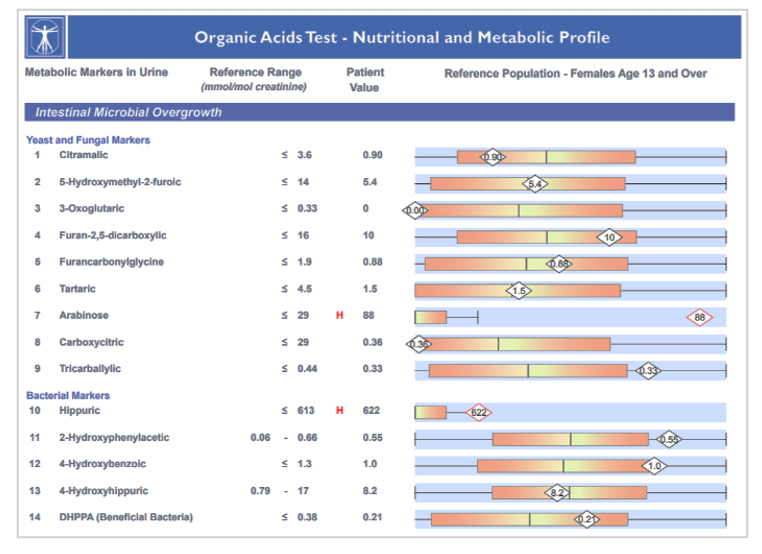 Among the circumstances that can benefit from an OAT analysis are skin conditions, fatigue, bloating and gas, headaches/migraines, inflammatory reactions, multiple chemical sensitivities, mood changes, nausea, poor blood sugar regulation and poor sleep[iv].
Among the circumstances that can benefit from an OAT analysis are skin conditions, fatigue, bloating and gas, headaches/migraines, inflammatory reactions, multiple chemical sensitivities, mood changes, nausea, poor blood sugar regulation and poor sleep[iv].
The patient agreed to have such a test done. The results indicated abnormally high levels of yeast and bacterial signatures. It also confirmed deficiencies in some B vitamins, glutathione and minerals.
Diet:
- Eliminate:
Alcohol, all refined starches and sugars, pasteurised dairy and all grains for a period of 6 weeks.
At this time, all fermented foods to be excluded as well. Limit coffee to one a day if not able to cut out completely.
- Include:
High nutritional value organic foods such as grass-fed meat, poultry, game and fish, eggs, brassicas, green leafy vegetables, herbs, spices and low GL veg and fruit. Fats and oils, nut butters, bone, fish and vegetable broths. Nuts and seeds in small amounts, only if pre-soaked overnight. Herbal teas of nettle, chamomile, fennel and tulsi.
The patient was encouraged to consult the low GL tool online and stick to low GL foods.
The plan is that, after the follow-up consultation and assessment of progress, the patient will re-introduce one excluded food item at a time and monitor reactions.
Supplements:
- A broad spectrum probiotic supplement plus a specific one for skin – Activated Probiotics’ “Biome Advanced” and “Breathe” were both prescribed in order to address the long-standing gut dysbiosis. The “Breathe” probiotic formulation from this range of probiotics addresses skin also.
- A multi-B complex – Cytoplan’s P5P in order to support the vitamin B insufficiency
- A Glutathione supplement – Cytoplan’s Cell-Active Glutathione Complex to support glutathione levels
- A quercetin and nettle complex – Viridian’s Quercetin B5 Plus Complex to help reduce allergenic reactivity
Bach flower remedy:
The Bach flower remedy Vine seemed to fit the patient best at this time due to domineering attitudes, inflexibility and overall rigidity. The patient was directed to take this for a week before she embarked on her recommended naturopathic programme.
Homeopathy:
Schüssler tissue salt Kali mur 6x twice a day on rising and retiring to support mucus elimination and reduce lymph stagnation.
Other naturopathic practices recommended:
- Bentonite clay external applications two to three times a week in order to support toxin elimination via the skin and reduce inflammation. The patient could use the bentonite on the breasts only, as a footbath or whole body mud pack.
- Dry body brushing daily on rising to help move the lymph and support elimination.
- Contrast showers were also recommended for the same reasons as the dry body brushing.
Follow-up
Patient returned for a follow up appointment in five weeks. She reported a significant reduction in all symptoms, to the extent that she had stopped taking the antihistamine prescription. She missed her wine and “pasta bolognese” but, as she had seen such drastic improvement, she was willing to stick to the regime. She reported two episodes of low blood sugar only one of which resulted in migraine. She also reported that she felt more relaxed and “at peace” and had not experienced any PMT at all. She was not keen on the dry skin brushing but loved contrast showers and bentonite packs, so she was happy to continue with those as well as the rest of the dietary and supplement regime for another six weeks. She also loved the Bach Vine remedy; “I tuck it in my bra when I do dressage, it helps keep me flexible”.
The patient had 3 more follow-up consultations which spanned a total of 21 weeks. During this period, certain foods were re-introduced: a little raw and fermented dairy, other fermented foods, fermented grains and pulses and the occasional glass of organic red wine. No further allergy symptoms, formication or low blood sugar symptoms returned. One bout of migraine was experienced after drinking red wine containing sulphites. Homeopathic Nux vomica 9x, 3 doses spaced 1hr apart, resolved this.
[i] Iris-organ correspondences:
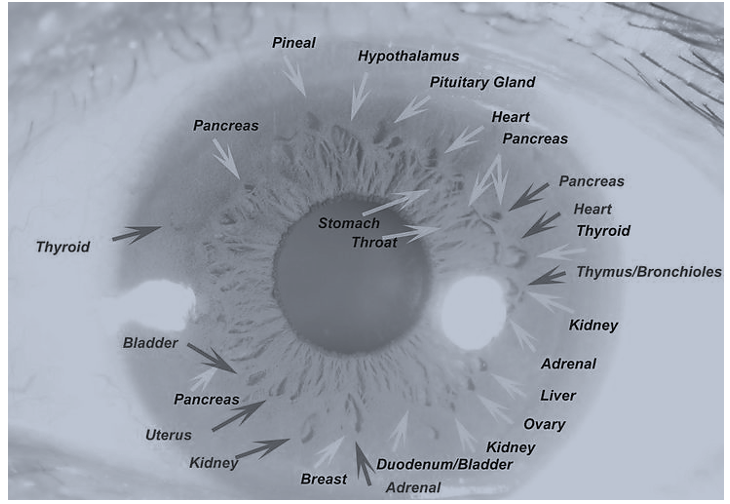 [ii] Ozand, Pinar. (2000). Hypoglycemia in association with various organic and amino acid disorders. Seminars in perinatology. 24. 172-93. 10.1053/sp.2000.6367.
[ii] Ozand, Pinar. (2000). Hypoglycemia in association with various organic and amino acid disorders. Seminars in perinatology. 24. 172-93. 10.1053/sp.2000.6367.
[iii] https://www.greatplainslaboratory.com/organic-acids-test
[iv] https://biodesignwellness.com/diagnosing-the-root-causes-of-illness-with-the-organic-acids-test/
National Lockdown Update – 6th January, 2021
The GNC has provided further guidance on the latest lockdown in England that became law on 6th January. The conditions for naturopathic practitioners to work are broadly the same as the November 2020 lockdown.
England
GNC members in England may work under the following conditions until the lockdown comes to an end or further conditions are embodied in law.
- GNC members are encouraged to carry out consultations remotely where possible.
- You can continue to provide your therapy, on a one-to-one basis to clients, for an identified mental or physical health condition or injury that is causing them pain, or having an adverse impact on their mobility or their quality of life. You must be able to evidence that your therapeutic intervention is supporting your client with their condition and record fully the condition, the treatment rationale and outcomes when available.
- You cannot provide treatment to a client in their own home unless you have received a direct referral from a statutorily regulated health professional.
- If your practice is based in your own home you can continue to work from there as long as it is COVID-secure and suitable PPE is used (see government guidelines)
- You should review guidance on using the Track and Trace app. (see here)
Scotland
- Scotland has entered full lockdown and are restricting the movement of everyone with a “stay at home” policy and severely curtailed travel radius.
The advisory is that no complementary medical approaches may be conducted if they are “hands-on“ but remote consultations are not covered and therefore acceptable. For more information, see here.
Northern Ireland
- Lockdown is scheduled to last until 6th February, 2021. The lockdown details may be seen here
- Close contact services, including well-being and holistic treatments, are not permitted to open. There is no restriction on close contact services relating to dental services, opticians, audiology services, chiropody, chiropractors, osteopaths, podiatry and other medical services, including services relating to mental health. For more information, see here
Wales
All of Wales is in lockdown alert level 4 – see here for details
- Most therapies are not permitted: “Close contact services – this includes beauty therapists, beauty advanced practices treatment practitioners, make-up artists, nail service technicians, reflexologists, aesthetics, holistic, wellbeing and other practitioners; acupuncture and electrocautery practitioners and massage therapists including sports and clinical massage therapists”
BUT there are some permitted exceptions to work: “Treatments or services which are providing medical treatments for illness or injury.
These would include therapists who are working alongside or in conjunction with a statutory regulated health professional – for example, a sports therapist based in a clinic owned by an osteopath, or working alongside doctors or nurses in a hospital or hospice to help support patients receiving medical treatment. Services that provide non-cosmetic laser / IPL medical treatment for illness or injury would also be permitted.”In all cases, the GNC recommends that members check with their professional indemnity insurers on cover.
Read More
Acute conditions respond very quickly to these remedies, supporting the immune system and accelerating the healing process. Chronic conditions respond at a more measured pace, according to the duration and severity of the disease or imbalance. Asthma, eczema, bowel problems, poor vitality due to toxin build-up, arthritis, hormone imbalance (and all the distressing symptoms that causes), allergies and so much more. In many instances, once the toxic load has been taken off the organs, the body will heal itself and no further intervention is required. Because this is a CORE THERAPY it can be used in conjunction with any other form of healing technique to enhance vitality and accelerate recovery.
So how do Homeobotanical remedies work?
The big question with all forms of treatment, medical and alternative is “do they really work or is it just the placebo effect?”
Current research and quantum physics is showing that everything is energy. So not only is it possible, but there is a strong possibility that energy healing is the healing of the future.
Many people report positive results from working with the remedies. Herbal remedies have been bringing healing relief to people for thousands of years.
In a study of 50 clinic cases submitted by six different clinicians, Homeobotanical therapy was shown to be effective in 75% of those cases.
Homeobotanicals have three distinct actions in the body:
Physical action includes organ drainage or stimulating the elimination of toxins from specific areas of the body. There is a nutritional component, which assists in the assimilation of minerals and other micronutrients.
Synergistic action which reinforces whatever other healing techniques are being employed as Hb’s maintain balance within the body.
The Dynamic action arises from homoeopathic potentisation and enables these remedies to directly stimulate healing within the body. The low potency adopted produces a gentle, sustained response resulting in remarkably few problems even in sensitive people.
Homoeobotanical remedies cover a comprehensive range of conditions. All remedies are mutually compatible and can be mixed in an infinite variety of ways to restore the health of a patient.
They work well with any other forms of healing including allopathic. Many Homoeopaths use Hbs to enhance their practice. You can add them to creams, gels, oils and add in Bach Flower remedies or any flower essence as well as homeopathic remedies to enhance the mix
|
|
Dear ANP Member
We hope your new year is getting off to a good start, and you were able to enjoy the holidays with friends and family.
As we start the New Year, we wanted to take the time to look back on what we achieved as an association together in 2021 and highlight some of our key goals for 2022.
Our members are the life and soul of our association, and in 2021 we had our best year to date, growing to over 3,000 practitioners.
We look forward to working with you closely in 2022 as we share our passion for natural medicine.
What we achieved in 2021
- Our online Naturopathic Summit was held with 20 keynote speakers and experts in the field of women’s health & hormones.
- The ANP Education Hub was launched to provide additional CPD content and an extensive webinar library for all your education needs.
- Mentoring was a key priority in 2021. We ran 25 different mentoring groups supporting our newly qualified practitioners in their transition to clinical practice.
- We contributed directly to The GNC on behalf of our members, paying their GNC registration fees, so our members didn’t have to pay any additional fees.
- We focused our attention on causes that are important to us, including transparency around covid-19 injections, health freedoms and natural immunity.
- We improved the tech of our website, including implementing automated GNC/ANP membership certificates, and started working with a SEO specialist on driving traffic to our practitioners’ directory profiles
- Our contraindication database was updated with the latest drugs, nutraceuticals and herbs
- We delivered 29 online CPD webinars for our members
What we will be working on in 2022
- Our new mentoring programme will be launched in January. This will include more structured learning for mentees, extra resources, along with better support to help our members be successful in clinical practice
- Implementing the feedback from our 2021 member surveys
- We are moving back to in-person events, both in London and regional areas. Keep an eye out for more events being launched in the next few months.
- Our in-person annual Naturopathic Summit will be on the 24th & 25th of September, 2022. We look forward to sharing our keynote speaker line-up with you soon.
- Our Naturopathy & Community Awards will continue throughout the year, and will feature the hard work of our members as we work to promote them within the community, making naturopathy more well known to the general public.
- We will continue our work with Private Health Insurance companies with the hope to integrate natural therapies into their policies
- We will continue to collaborate with our key partner associations, including the IMA, IHC and GNC, and look to establish a referral system for our members.
- Lastly, while the last few years have left us feeling isolated and out of touch, we are hoping that this year will bring us together, and as such we are looking to do more member outreach and networking so we can understand the needs of our members better, and work together on a united front.
|
|
Dear ANP Member
We hope your new year is getting off to a good start, and you were able to enjoy the holidays with friends and family.
As we start the New Year, we wanted to take the time to look back on what we achieved as an association together in 2021 and highlight some of our key goals for 2022.
Our members are the life and soul of our association, and in 2021 we had our best year to date, growing to over 3,000 practitioners.
We look forward to working with you closely in 2022 as we share our passion for natural medicine.
What we achieved in 2021
- Our online Naturopathic Summit was held with 20 keynote speakers and experts in the field of women’s health & hormones.
- The ANP Education Hub was launched to provide additional CPD content and an extensive webinar library for all your education needs.
- Mentoring was a key priority in 2021. We ran 25 different mentoring groups supporting our newly qualified practitioners in their transition to clinical practice.
- We contributed directly to The GNC on behalf of our members, paying their GNC registration fees, so our members didn’t have to pay any additional fees.
- We focused our attention on causes that are important to us, including transparency around covid-19 injections, health freedoms and natural immunity.
- We improved the tech of our website, including implementing automated GNC/ANP membership certificates, and started working with a SEO specialist on driving traffic to our practitioners’ directory profiles
- Our contraindication database was updated with the latest drugs, nutraceuticals and herbs
- We delivered 29 online CPD webinars for our members
What we will be working on in 2022
- Our new mentoring programme will be launched in January. This will include more structured learning for mentees, extra resources, along with better support to help our members be successful in clinical practice
- Implementing the feedback from our 2021 member surveys
- We are moving back to in-person events, both in London and regional areas. Keep an eye out for more events being launched in the next few months.
- Our in-person annual Naturopathic Summit will be on the 24th & 25th of September, 2022. We look forward to sharing our keynote speaker line-up with you soon.
- Our Naturopathy & Community Awards will continue throughout the year, and will feature the hard work of our members as we work to promote them within the community, making naturopathy more well known to the general public.
- We will continue our work with Private Health Insurance companies with the hope to integrate natural therapies into their policies
- We will continue to collaborate with our key partner associations, including the IMA, IHC and GNC, and look to establish a referral system for our members.
- Lastly, while the last few years have left us feeling isolated and out of touch, we are hoping that this year will bring us together, and as such we are looking to do more member outreach and networking so we can understand the needs of our members better, and work together on a united front.